Americans today associate PTSD with our Iraq and Afghanistan veterans. Truly, post-war trauma must have always been with us. We are, after all, human and violence of any kind offends us, especially when life and limb are violated. But in the Great War, more men survived the realities of bullets, shrapnel, gas and chemical attacks as well as disease than in any other war. The reason is, of course, that we had organized medical teams behind the lines at the ready.
True that those teams had little in the way of medicines or technology to aid them in rapid response to aiding wounded. But the process of getting aid to a wounded soldier had begun.
What do we know of that process?
1. Speed
We learned that the sooner a medical team sees a man, they can not only bandage him and/or administer first aid, but ease his pain.
The need for speed meant armies developed the concept of stretcher bearers who carried wounded from the line backward to a first aid station. This may have been a TRIAGE station where wounded were assessed for survivability. Triage posts were often served by ambulances, either horse drawn or mechanized. These vehicles ran over rough terrain at slow speeds and men inside often had no morphine or other to ease their pain.
Analysis of wounded men immediately behind
fighting line was often called TRIAGE, or separation
of wounded in to 3 groups. This was: 1. those who
would not live no matter the medical attention; 2. those who needed
immediate attention; 3. those who could wait a reasonable time for attention.
2. Efficiencies
We learned that a proper supply of emergency materials was necessary the closer to the front a medical team operated. This included not only scissors, bandages, splints, gauze, but also fresh sterile water, iodine and other similar sterilizing ointments.
 |
This picture in a church in a Field Hospital shows either
primary or secondary line treatment. This is June 1918 and could
be primary treatment, if behind a rapidly advancing or retreating
front line. |
3. Understanding of infection
The Great War occurred during a period when medical researchers were first beginning to understand the process of bacterial infection and how to limit its virulence. No antibiotics were yet available. So cleansing a wound was a laborious process. Furthermore, the forensics of bullet trajectories and the erratic intrusions of shrapnel made removal of such foreign objects more of a guessing process than a logical one.
X-rays were available but limited in their scope. Furthermore, not every medical team had use of one.
4. Psychological effects of exposure to elements
Not only was a soldier exposed to bombs, bullets, shrapnel, gas and chemicals, he was exposed to the actions and reactions of his comrades to these elements. Add to that the primitive conditions of living and working in knee deep mud, poor hygiene, poor diet and constant pressure to perform menial tasks, and the average soldier suffered physical and social challenges which few current-day non-combatants can identify with.
5
. Secondary surgery and recuperative treatments
Often a wounded man required one or more secondary surgeries. Operations performed by medical teams close to the fighting lines were under their own pressures to work quickly. This could mean the wounded had received life-saving treatment but required advanced surgeries to enhance the primary surgery.
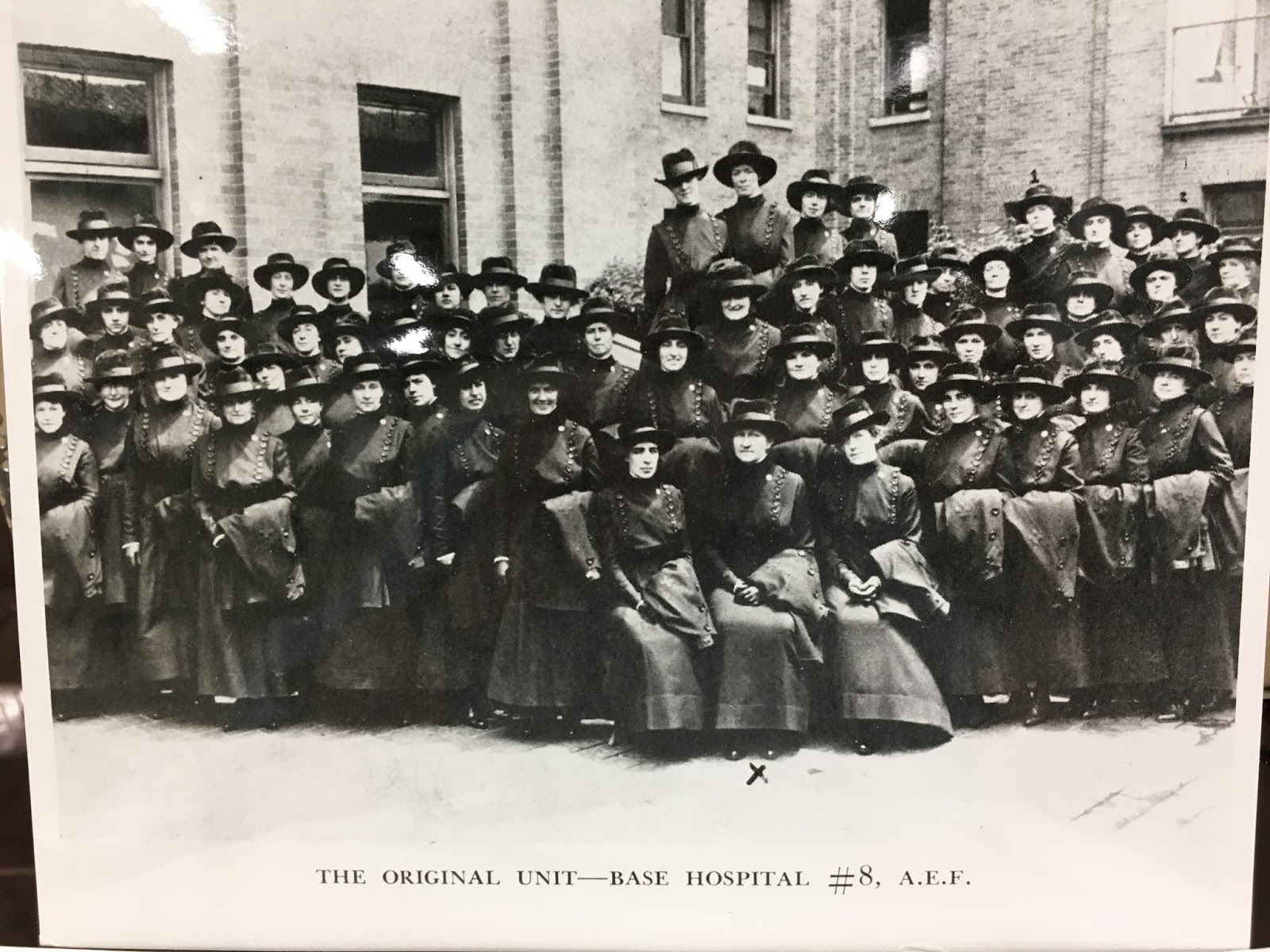
To ensure continued care in a more secure area, the US Army (like other armies in this conflict) established hospitals well behind the lines. Americans established a base hospital system, staffed by entire teams from hospitals in the continental US and complemented by others from other area who joined those teams. These base hospitals were approximately 50 to 100 miles behind any front. So indeed a wounded man was transported even farther back of the line to a stationary base from which he could recuperate for an extended period. He was either certified completely recovered and returned to the front lines to fight again or sent on down the line to return home. In the US, he could be treated at another hospital or returned to his civilian home.
No such entity as our current Veterans Administration existed at that time. A man was left to recuperate on his own. The VA was a post World War II entity created by the Congress.
 |
Facsimilie of facial wound prosthetic
Musee de la Grande Guerre, Meaux, FR
Jo-Ann Power photo |
6. Rehabilitative services which were new
 |
Torso back brace and amputee of leg prosthetic.
Musee de la Grande Guerre, Meaux, Fr
Jo-Ann Power photo |
Physical therapy as a professional service was a new technique offered to amputees and those who had suffered physical incapacities. Much of this kind of therapy included training for new professions, such as weaving and metallurgy. For those men who were amputees, many were offered prosthetic devices for arms and legs.
For those men who suffered facial deformities, plastic surgery was in its primary stages of development. And while many of these men opted to go into "retirement homes" because they did not wish to re-enter society, many of them volunteered to receive prosthetic masks. Many volunteered to be patients in novel procedures which today form the bedrock of our knowledge about efficacies in plastic surgery.
 |
Arm-shoulder prosthesis
Musee de la Grande Guerre, Meaux, FR
Jo-Ann Power Photo |
For more on plastic surgery, visit:
http://www.bbc.co.uk/guides/zxw42hv
For more on emotional trauma, shell shock and PTSD, visit:
http://armsandthemedicalman.wordpress.com
 |
| Frontispiece of Pickerill's text on facial surgery, produced on the basis of his M.S. thesis to the University of Birmingham |















_369th_Infantry_(old_15th_National_Guard_of_New_York_Cit_._._._-_NARA_-_533553.tif.jpg)






_13_September_(black_line).jpg)









